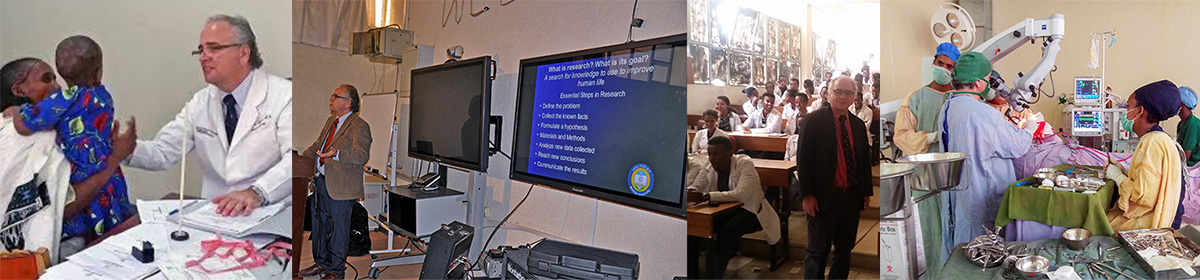
The author assisted by a Mekelle University neurosurgery resident performing microscopic brain tumor resection at Ayder Hospital in 2018
The neurosurgical team of Mekelle University’s Ayder Hospital struggles to save the life of a poor farmer from a deadly brain tumor. A critically ill patient who faced death unless he underwent emergent brain surgery. An intense multi-hour confrontation with a brain tumor. This became an almost everyday occurrence for our team.
I had come to Ayder Comprehensive Specialized Hospital in Mekelle, Ethiopia in 2015 to start a neurosurgery program. This was a federal teaching teaching hospital and part of a university medical center serving about 15 million people. We wanted to create a sustainable medical service that also train neurosurgeons.
As the family said goodbye to him he left the ICU for the operating room. He had been intubated and resuscitated in the emergency room where he presented with coma. A young uneducated farmer from a remote primitive area who had been deteriorating for a year and half. Tumors in this part of the world are large and angry because they present so late.
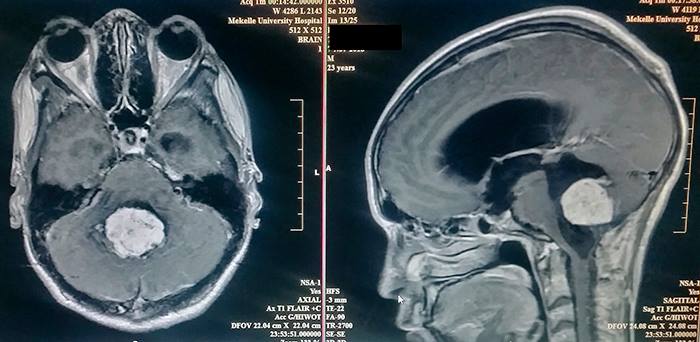
A large 4th ventricle tumor next to vital structure would be difficult to remove
The MRI of the brain showed a 10 centimeter ependymoma in the fourth ventricle which was highly vascularized. This is the type of case neurosurgeons dream of, a mix of danger and hope.
The residents and fellows do the initial opening until the back of the brain is exposed which takes the first hour of surgery. I can see the tumor erupting to surface with very swollen blood vessels around it. Instead of the ependymoma (an easier tumor to remove) this was going to be hard. I begin working a millimeter at a time. Gently dissecting tumor from brain, isolating and separating scar bands and blood vessels. Using directed light and magnification for the next 8 hours I cannot take even a 5 minute break. Removing the tumor means there is constant blood loss. The brain receives more blood than any other organ. Tumors cause extra blood vessels to grow into them. As you control one bleeder another 2 start.
By the fourth hour into surgery he has lost 5 liters of blood and his blood pressure is fragile. By the sixth hours there is still about 20% of the tumor left which is covering the cerebral aqueduct. This must be removed to allow flow of cerebrospinal fluid. We are millimeters away from vital areas that cannot be damaged.
Another 2 hours goes by and there are times when the blood loss starts again and pressure gets low even with another 2 units. After 8 hours from the beginning of my part of the surgery the tumor is completely removed. The patients blood pressure is holding thanks to high dose epinephrine (a drug to raise blood pressure in critical patient). Now comes the hardest time. Will the patient wake up? He goes to the intensive care unit and we wait. After a few hours he begins to move in a way that suggest he will emerge from coma.
This is the life of neurosurgeon. Fighting to stay on the brink of life for hours at a time.
The $26 million investment by Velocity in Mekelle which was 70% funded by loan from the Development Bank of Ethiopia was a total loss due to destruction by the ENDF and Eritrean forces. Thousands of jobs and loan repayment are gone.
Abiy Ahmed and Esaias Afwerki beserk destruction destroyed thousands of workers lives, millions in foreign investment, and cancelled the future repayment of millions of dollars in loans made by the Development Bank of Ethiopia to foreign investors in Tigray. The false message of liberation of the Tigray from the TPLF by Abiy Ahmed’s genocide which continues today was countered by some like Abera Niguse in the interim administration of occupation. Now with carpet bombardment of Amhara killing thousands of civilians and businesses, the Abiy Ahmed war machine continues the same in Amhara.
The false message of liberation of the Tigray from the TPLF by Abiy Ahmed’s genocide which continues today was countered by some like Abera Niguse in the interim administration of occupation. Niguse appointed as Head of the Bureau of Justice for the Tigray Interim Administration during the Ethiopian occupation complained in February 2021 that the destruction of factories and businesses in Tigray was illegal. He noted that the procedure undertaken was a “law enforcement operation” that should not have constituted mass destruction in a radio broadcast on FM 104.4 in Mekelle. The damage done would require an investment of over 100 billion birr to repair he stated. Essentially every factory and business including pharmaceuticals, construction, mining, truck and agricultural equipment manufacturing, garments, steel, poultry, farming, cement production, etc. was destroyed.
I was involved in trying to help Velocity, an Indian and Dubai based garment company in Mekelle which also produced oxygen for industrial use, be allowed to produce medical oxygen but instead Eritreans were allowed to destroy the factory and take components to Asmara. The Velocity investment in Mekelle was $26 million dollars with a 70% loan from the Development Bank of Ethiopia. Now thanks to Abiy Ahmed’s destructive mania thousands lost jobs and loans outstanding to the Development Bank of Ethiopia will never be paid. This is just one example of many examples of how Abiy Ahmed’s will ultimately help break the economy of Ethiopia.
Niguse complained “This is not about getting rid of TPLF or capturing some clique. This war had no discipline. It has created insurmountable social and economical issues for the foreseeable future for the people of Tigray. It has caused serious insecurity in the region. Tigrayans are abused and suffering. Churches are burning. Women and young girls are being raped. Improper house checks and raids. All types of machinery, cars and many other properties of Tigray have been looted and taken out of the country’s border, some are taken to central Ethiopia”.
In April 2018 Abiy Ahmed the new appointed Prime Minister of Ethiopia came to visit Mekelle, the capital of Tigray, with a message of hope, cooperation, and development. As a teenager in the Ethiopian Army he had served in the Tigray region and learned Tigrinya, the native language. He watched a circus show, sat with Tigray People Liberation Front leaders, and talked about a future together. Before his visit he had stated that it was time for a new era for all regions to work together. That the country should look forward and not be focused in the past.
Abiy Ahmed sits with TPLF leaders at the Mekelle Monument to Martyrs
He talked about infrastructure development including hydroelectric dams, a railroad project, the Mekelle water problem, giving support to private sector development , loans for investment, export support from the national bank, improving tourism, bringing public meter taxi for Mekelle, and a short lease proclamation for agriculture. None of these things ever happened.
Instead after his visit there came to be a movement in Ethiopia about the need to deal with the past. In late 2018, the Prime Minister created a Reconciliation Commission “to maintain peace justice, national unity and consensus as well as Reconciliation among Ethiopian Peoples.”
Discussion began about injustice under the Monarchy, the Derg, and the Ethiopian Peoples Democratic Front under whose auspices Abiy Ahmed came to power as a compromise between Amhara and Oromia factions. Soon however, this effort which lacked any clear mandate, become a mechanism for consolidating power.
By the 2019 budgets for the Tigray state which were calculated by population formulas used for all regions were beginning to be cut. Many former political leaders including those of the TPLF were sought out for arrest. Ethnic identity in the Amhara region, and other regions as well, which normally had about 10% Tigray became an issue. There were pushes which began subtilty but then became open and forceful causing many Tigray to leave other regions and move back to Tigray. Abiy Ahmed was using the usual formula for dictators by creating a Tigray strawman. He began to turn on even those who facilitated his rise namely Jawar Mohammed from Oromia.
On the occasion of the 2019 harvest and women’s festival Ashenda , Abiy Ahmed sent a message that Tigray culture was an important and vital part of Ethiopia. In a speech to Parliament he stated that the TPLF and Tigray leadership were examples to follow for other regions in Ethiopia.
The Tigray Ethiopia conflict which was the end result of almost two years of escalating actions against the Tigrayan ethnicity was touted as a “law enforcement action”. That the Ethiopian government was going to free the Tegaru people from the crimes committed against them by the TPLF. Instead with its expatriate Eritrean allies it looted, killed, raped, and stole from the very people Abiy Ahmed said he would “liberate”. Finally he sarcastically complained that he had to remove his army from Mekelle because the Tegaru were helping the Tigray government too much.
Today more than 300,000 Tegaru are suffering famine. Aid is being actively blocked by the Ethiopian government. Revolts are now active in Beningshagul, Afar, Oromia, Agew, Somali, and Gambella who also feel betrayed. Hope has been replaced to a fight for survival against a great betrayal.
Ayder Comprehensive Specialized Hospital campus of Mekelle University
Every once in a while I receive audio communication from Mekelle. This was a summary of what they told me of the situation on August 19,2021. Starvation, lack of healthcare, and the continuing blockade to help the situation continue.
Ayder Comprehensive Specialized Hospital of Mekelle University
This is normally the tertiary hospital for Tigray and surrounding regions having a catchment area of about 10 million. It is part of the second largest medical school, research center, and training center for medical specialties in Ethiopia. Although civil non-violent actions stopped complete destruction of the hospital by Eritrean and Ethiopian National Defense Forces the hospital now is almost at a standstill. Having no antibiotics, no insulin, no cancer medications, cardiac medications, working ICU, no c-section or blood transfusion for delivery, no ambulance service the population of Tigray has been rendered to having essentially without healthcare. No laboratory equipment, x-ray machine, anesthesia machines work anywhere in Tigray. From smaller hospitals most of the equipment was taken as war booty to Eritrea. Many hospital were ransacked and bombarded by artillery. There is very little diesel available to run the hospital generator.
Currently the hospital being overwhelmed with many patients lying in hall ways with starvation victims. Children especially are the most vulnerable so they make the majority of victims. There are outbreaks also of COVID-19 and other viral diseases because no immunizations are available. Recent outbreaks of rabies have occurred because hungry vicious dogs are roaming the streets. Ayder has no rabies treatment available. There is only few intravenous bags left and those are being used to try to help infant and child victims of starvation. There is now a World Health Organization team in place to assess and assist but their pleas for help are ignored by the Ethiopian government.
Everyday more victims of abuse both male and female are coming to the hospital for counseling and care. High numbers of families are disconnected from others trying to find their loved ones.
The staff and physicians of the hospital and university have not been paid for three months. The food supply is gradually deteriorating and is much worse in the countryside. Ethiopia blocked planting and killed livestock during the occupation of Mekelle. Stores of seeds, fertilizer, farming equipment were taken as war booty to Eritrea.
Condition of the Tigray Power Supply -19August 19, 2021 Electric power remains out in all of Tigray. There is a very sparse supply of fuel for any generators and when available it comes at a high price.
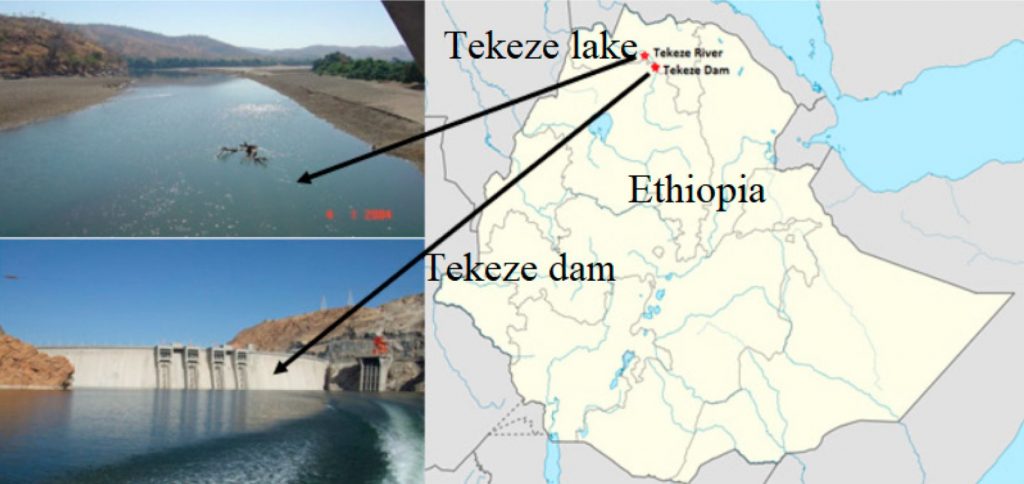
The Tekezé Dam normally has four turbines that produce 300 mw of electricity through a 105 kilometer transmission line to Mekelle. It was severely damaged by the Ethiopian National Defense Force and Eritrean forces leading up and during their occupation of eastern Tigray. Now I am informed that work is going on to at least partially repair the damage. Apparently the current water level is not high enough to make use of what is currently functional so they are hoping with more time the level may rise. Significant components need to be replaced but this blocked by the Ethiopian blockade. They are hoping some interim repairs will allow partial function when the water level rises from the rainy season.
The Tekezé Dam was attacked and rendered nonfunctional by Eritrean and Ethiopian National Defense Forces
The Ashegoda wind project was similarly sabotaged by Eritrean and Ethiopian National Defense Forces. This wind farm close to the Mekelle airport can produce 120 MW power out of 30 turbines that can meet the needs of 3 million people in Tigray. I am informed that vital parts have been damaged or stolen and then taken to Eritrea. In order to repair these vital structures supplies and expertise must be allowed past the current Ethiopian blockade.
In the face of terrible civilian atrocities done to the Tigray people by the invading Ethiopian National Defense Force, Amhara militias, Eritrean military, and Somali mercenaries there are increasing reports of mercy and kindness given to their attackers by Christians and Muslims.
The city of Hawzen in peaceful times
The city and villages surrounding Hawzen have been the victim of attack first in 1988 at a market place where hundreds of civilians where massacred and again this Spring. The following is an eyewitness account (corrected for grammatically errors) of mercy in the face of horror:
“Last March near Hawzen there were joint offensive attacks against TDF by both Eritrean and Ethiopian forces with heavily mechanized army targeting civilians. The TDF waited them in a very strategic place to counterattack which caused the enemy to be dispersed. Some of the enemy soldiers were captured by farmers who had seen friends and family cut down by enemy fire while they was trying to hide themselves around their village. The farmers held them and the soldiers started to cry …one soldier said that they deserved even death punishment but he pleaded to the farmer to be taken and killed in front of the church in order to save his body from being consumed by vulture or hyena. But the farmers were with full of humanity and mercy, they gave food and taken to POW center with out any harm.”
Here is another account from a village near Mekelle”
“In wejerat ..it is just east of mekelle. One farmer is killed by Ethiopian soldier and immediately some the attacking soldiers captured and taken to to show to the victim’s family what the soldier had done. But the family of the victim told to TDF to not harm them …since they have a family like us ..we dont need a bad thing on them we need only a verdict from God”….
Tigray Defense Forces meet with representatives of a captured city in Amhara
In the attached picture TDF talks to gathered Amhara of a captured city to reassure them that their everyday life can continue under their local leaders.
The government of Ethiopia while claiming a law enforcement operation has committed genocide to the people of Tigray and turned Tigray into a concentration camp.
What is the definition of a concentration camp?
According to the highly respected encyclopedia Britannica a concentration camp is “defined as an internment centre for political prisoners and members of national or minority groups who are confined for reasons of state security, exploitation, or punishment, usually by executive decree or military order”. What the Ethiopian government has done to the Tegaru, Irob, Agaw, Kunami, Afar, Orthodox, Catholic, Christian, and Muslims who live in Tigray meets every requirement stated in this definition of a concentration camp and in every way just a deadly as those recalled from previous examples when evil predominated a society.
Actions of Ethiopia against Tigray are more than law enforcement
When the Ethiopian National Defense Forces and Eritrean Army units invaded the Regional National State of Tigray in November 2020 the leadership of Ethiopia specifically stated that was being undertaken was a law enforcement action to capture the leaders of a “terrorist group”, Tigray People’s Liberation Front (TPLF), and that there was no intent to take action against the civilians of Tigray. In fact they explicitly stated they were proceeding with this invasion to not only capture the leadership but also to protect the security and life of their “brother” Ethiopians.
At the time of invasion I was Chief of Neurosurgery and on the faculty of Mekelle University, a federal university not under the Tigray state, which had medical students and specialty trainees from almost every regional state in Ethiopia as well as surrounding countries. Additionally it administered Ayder Comprehensive Specialized Hospital which served a population of about 10 million including not only Tigray but also Afar, northern Amhara, and recently even Eritrea intermittently when the border was open. Additionally we occasionally cared for patients from Addis Ababa and the SNNP (Southern Ethiopia).
Following the complete take over of Tigray we were initially told by the Interim government and military commands that the government, medical, and educational services would be quickly restored. But instead they quickly deteriorated well before the reorganization and re-emergence of the Tigray Defense Forces. Except for a very short time of a few weeks early on the following have been cut-off and never restarted including banking services, electricity, telephone and cell, internet, water, civil infrastructure management, hospital supply, schooling, etc.
Although the Federal government claimed it was giving 70% of the trickle of very basic aid that was coming in reviews by well established international authorities revealed it was less than 3% of the total which was in itself dramatically less than required.
Soldiers of the Ethiopian Army even took videos celebrating the killing of civilians
As the weeks progressed the undeniable evidence was increasingly seen that sexual abuse of women now estimated to be in the thousands, extra judicial killing of whole villages, routine execution of males even those below or above that generally considered to be militarily capable were reported even by the Ethiopian Human Rights Commission. Although there may be a possibility of some actions by Tigray militia which also require investigation the exponentially greater magnitude affecting hundreds of thousands of violation of human rights and killing by soldiers under the direct command of the Ethiopian government cannot be denied. If not stopped the number being threatened will rapidly accelerate to millions.
More than 350,00 people are at critical levels of starvation now and will increase rapidly
Instead of taking corrective action to improve the humanitarian situation which would possibly yield the benefit of making the civilian population of Tigray more peaceful instead new arguments surfaced from mouthpieces of the Prime Minister’s advisors that due to previous claims of unfair treatment by the TPLF that justified the violations of human rights currently underway. Videos emerged stating that every Tigray should be killed at birth. Eritrean and ENDF soldiers have stated to neutral third parties that they were instructed to rape women to destroy the chance for Tigray to have children.
The Nejashi Mosque was bombarded and then ransacked
Religious institutions, artifacts, and worshipers were targeted for destruction which had nothing to do with a “law enforcement” action. One of the most important Mosques in the world in Negash where the followers of Mohammed took refuge from prosecution from pagan Saudi rulers at the invitation of a Christian king was intentionally bombed and ransacked. What does that have to do with “law enforcement”? Monasteries in Western Tigray with religious texts hundreds of years old were attacked with their treasures destroyed and clergy assassinated. The ancient Ethiopian Orthodox Church which traces its roots to the early Jewish religion of Menelik I and then the Christian kingdom of Ezana in Axum was desecrated with the murder of at least 80 unarmed worshipping civilians. What does that have to do with “law enforcement”?.
Aksum’s Our Lady Mary of Zion Church where Eritrean soldiers killed civilians
It is well documented that Eritreans, ENDF, and Somali mercenaries destroyed factories and businesses including those of foreign investors who generated income for the Ethiopian government and provided employment for civilians. Many pieces of equipment of not only these but also the national Ethio-telecom company were taken by Eritreans as war bounty to Eritrea. How does this destruction of Ethiopian federal property qualify as “law enforcement”?
The invading forces were instructed to destroy seeds and prevent farmers from planting crops. Many livestock were killed to be consumed by no one or taken to Eritrea in trucks. Both aid and commercial food supplies where blocked from entry to Tigray. Gradually both the Federal Government and the government of Amhara began to change their tune to explain this by saying that the population of Tigray was too supportive of the TDF and that NGOs were smuggling weapons with the aid. They accused organizations with much greater long standing reputations of wrong doing with no evidence instead trying to cover their own genocidal intent.
The government of Ethiopia as late as 2019 was a signatory to the Genocide Convention of the United Nations which states verbatim any of the following acts committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group, as such:
Killing members of the group;
Causing serious bodily or mental harm to members of the group;
Deliberately inflicting on the group conditions of life calculated to bring about its physical destruction in whole or in part;
Imposing measures intended to prevent births within the group;
Forcibly transferring children of the group to another group.
The treaty recognizes the following two elements of the crime
A mental element: the “intent to destroy, in whole or in part, a national, ethnical, racial or religious group, as such”; and
A physical element, which includes the following five acts, enumerated exhaustively:
Killing members of the group
Causing serious bodily or mental harm to members of the group
Deliberately inflicting on the group conditions of life calculated to bring about its physical destruction in whole or in part
Imposing measures intended to prevent births within the group
Forcibly transferring children of the group to another group
Shows Ayder Hospital and the streets lining it where a brave protest occurred
How a community of different faiths and ethnicities came together to save their hospital, Ayder Comprehensive Specialized Hospital, in the city of Mekelle, Tigray region of Ethiopia in the face of a horrific invasion by Ethiopian National Defense and Eritrean forces. In the previous post I described the culmination of events that deterred the ransacking. Here I will tell the story of how it began.
I have gathered some more information on how the heroic unarmed resistance began to stop pilfering and ransacking of Ayder Comprehensive Specialized Hospital in Mekelle from the occupying Ethiopian National Defense Forces and Eritreans.
The Adishmdhun mosque where the muazzin made a call to action
Among the first to call citizens to action was the muazzin of the Adishmdhun Mosque. Although there was no electricity in the city using the mosque generator and microphone he called people to guard the hospital. The message was ” to all residents of Mekelle be Muslim, Christian, males or females : Ayder is being looted, so go and protect your hospital “. Immediately the people began to make the gatherings. There was was a group of motorcycle men who tended to gather at a pub just a few blocks from the hospital who began calling the same thing using a speaker. Youth groups and community elders answered the call. The demonstration and blocking of the roads was done with people of all faiths and different ethnicities.
The Nejashi mosque in Tigray was bombed and looted
The Muslim community would later hear about the desecration of the Nejashi mosque in Tigray by ENDF and Eritrean forces. This mosque is particularly significant as it was founded by the first followers of the Prophet Mohammed (Peace be upon him) who were given refuge in Ethiopia from the pagan Saudi rulers.
Throughout the occupation young men volunteered to patrol the streets around the hospital in defiance of the night time curfew pronounced by the ENDF and the Eritreans. Unfortunately some were shot and killed on sight. How many we do not know yet. Sometimes the body was just taken away so that relatives do not know what happened to them.
Shows Ayder Hospital and the streets lining it where a brave protest took place. Pictures I had of the events described were erased by Eritrean patrols that would search me everyday I went to the hospital I will never forget the bravery of the people in Mekelle who unarmed defended their hospital. This picture shows the streets around Ayder Hospital where it all happened.
This is the story I witnessed of the brave unarmed civilians peacefully protesting and blocking invading forces from ransacking Ayder Comprehensive Specialized Hospital in Mekelle, Ethiopia in November of 2020. I had been performing neurosurgery, teaching fellows, and medical students at Mekelle University in the Tigray region of Ethiopia since 2015 in a federal university and hospital. As such I was present in Mekelle from the onset of the war between the Tigray Defense Force and the Ethiopian/Eritrean forces from the onset until my evacuation near the end of December 2020 at the behest of international influence and my family which was three days of driving through multiple checkpoints and unstable areas until we finally arrived in Addis Ababa.
Following the retaking of Mekelle by the Tigray Defense on June 28, 2021 there has been a mixture of sadness and joy. For sometime I have wanted to tell the story of what I think was the most heroic thing I have ever seen in my life which was the unarmed defense of Ayder Comprehensive Specialized Hospital in Mekelle. Prior to this time I felt telling it would result in reprisal to the citizens of Mekelle. Now that Mekelle is free it is important to tell it.
For almost 24 hours on November 25, 2020 the city of Mekelle was attacked constantly by artillery, rocket attack, and airstrikes even though the Tigray Defense Forces had left the city to only civilians. In my own immediate neighborhood just a few blocks from the Mekelle University hospital, Ayder Comprehensive Specialized Hospital many homes and buildings were destroyed and many killed. A market and home for elders was directly hit killing and wounding many.
About 200 yards from my house, a home that housed a large extended family suffered a direct hit that sent shrapnel breaking my windows at about 6:30 in the morning. I ran over there to find a young woman in the street with a severe bleeding wound in upper leg but that was just the beginning of the horror. The walls of the house had been destroyed on two sides and the rest looked like a Swiss cheese with many perforations. On the ground was a motionless young woman who had only a red spot on the ground where her chest was supposed to be. Her lifeless arms were extended with each one holding toddlers. The children where crying. When I pulled back their hair I found that hundreds of small munitions fragments had penetrated the scalp of both children although the eyes seemed okay. There was nothing we could do for the mother nor her mother who lay beside her dead as well from penetrating shrapnel. Remaining family members rushed the sister with the injured leg and the children to Ayder Comprehensive Specialized Hospital.
At the hospital emergency room there was wave after wave of ambulances and private vehicles bringing those hit by the attack who were all civilians. Some could be helped but many were beyond hope. We were able to save the children and their aunt from the attack near my house. Although we would sometimes previously do mass casualty from bus accidents in the past this was a much greater magnitude as we saw more then 120 patients in the first few hours.
Before the invasion of the city, we had been receiving civilian causalities, Tigray Defense Force causalities, and also Federal/Eritrean causalities. We treated them all the same. The local people even brought food and blankets for the all the groups. However after the invasion the tenor of the invading force changed. Many patients were just suddenly whisked away to parts unknown and we were not allowed to inquire.
The next day on November 26, 2020 at which time Federal Ethiopian armed forces and Eritrean forces invaded unopposed the city of Mekelle. For the next few days in Mekelle there were Ethiopian and Eritrean forces looting, shooting, robbing, and harassing civilians all around the Ayder area where I lived and the hospital was located. The hospital was occupied by Ethiopian army regulars, then Special Forces from Oromia, and so-called Federal Police. Then suddenly for about half a day they disappeared.
Rumors where flying in the city that Eritreans where ransacking public utilities, schools, etc. The hospital had always been a source of pride and necessity for not only Mekelle but all of Tigray. The local population of civilians began to put tires, logs, and stones to block trucks or other vehicles in the streets surrounding around Ayder Comprehensive Specialized Hospital, the main teaching and tertiary hospital for Tigray, fearing that the hospital which was highly valued by the city would be destroyed or looted. Special Red caped soldiers showed up and began harassing the locals more and more.
The locals did not back off. They gathered by the thousands and began to surround the hospital 24 hours a day. Many times semitrucks and smaller trucks driven by Eritreans which were empty tried to make it to the hospital to loot it but where physically blocked by protestors standing in their way. At one point a group of young men were shouting about ten feet in front me to the soldiers. Suddenly the soldiers fired at them killed one and injuring two others. At that time there were tires burning all around the hospital with thousands of protesters. The soldiers were scared and I feared the worst was going to happen. It was tense until morning. Finally the lined up trucks driven by plain clothed Eritreans were told to leave by the invading forces. The two that survived to be treated were hauled off from the hospital by the invading forces and have not been seen again as far as I know.
Pictures I had of the event were erased by Eritrean patrols that would search me everyday I went to the hospital but I will never forget the bravery of the people in Mekelle who unarmed defended their hospital.
The Department of Neurosurgery at Ayder Comprehensive Specialized Hospital of Mekelle University treats over 1000 significant head injuries every year including performing an average of 2.5 operations per day. All patients should undergo standard multiple trauma resuscitation and assessment by Advanced Trauma Life Support Guideline.
Since 2015 the Department of Neurosurgery at Mekelle University has instituted a standard head injury protocol (now revised in 2019) for the assessment and treatment of children and adults at Ayder Comprehensive Specialized Hospital based in part upon the local settings of Northern Ethiopia and the international guidelines including that of the Brain Trauma Foundation
Intracranial pressure monitoring is not economically feasible in Ethiopia but we are developing research protocols to look at optic nerve sheath diameter by serial ultrasound in the near future.
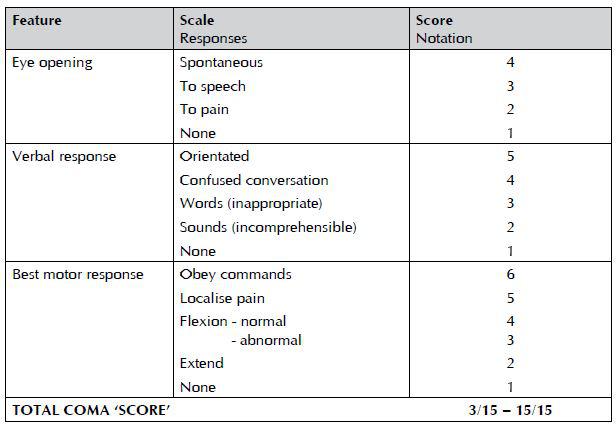
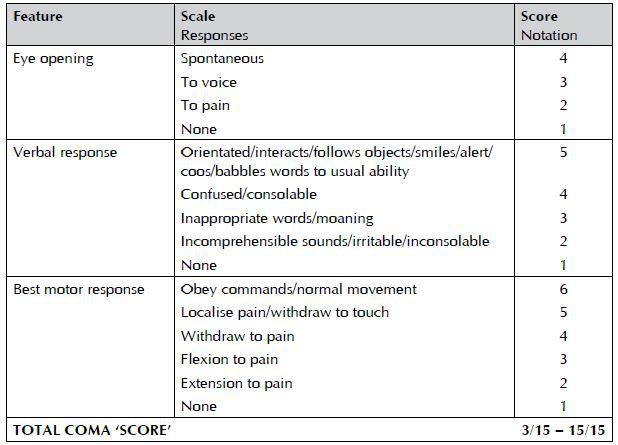
Adults Initial Assessment The management of patients with a head injury should be guided by clinical assessments and protocols based on the Glasgow Coma Scale and Glasgow Coma Scale Score.
Adult Glasgow Coma Scale
Indications for referral to hospital Adult patients with any of the following signs and symptoms should be referred to an appropriate hospital for further assessment of potential brain injury:
1. GCS<15 at initial assessment (if this is thought to be alcohol related observe for two hours and refer if GCS score remains<15 after this time)
post-traumatic seizure (generalized or focal) focal neurological signs
2. signs of a skull fracture (including cerebrospinal fluid from nose or ears,
hemotympanum, boggy hematoma, post auricular or periorbital bruising)
3. loss of consciousness
4. severe and persistent headache
5. post-traumatic amnesia >5 minutesrepeated vomiting (two or more occasions)
6. retrograde amnesia >30 minutes
7. high risk mechanism of injury (road traffic accident, significant fall)
coagulopathy, whether drug-induced or otherwise.
Indications for head CT scan Immediate CT scanning should be done in an adult patient who has any of the following features:
1. eye opening only to pain or not conversing (GCS 12/15 or less)
2. confusion or drowsiness (GCS 13/15 or 14/15) followed by failure to improve within at most one hour of clinical observation or within two hours of injury (whether or not intoxication from drugs or alcohol is a possible contributory factor)
3. base of skull or depressed skull fracture and/or suspected penetrating injuries
4. a deteriorating level of consciousness or new focal neurological signs
full consciousness (GCS 15/15) with no fracture but other features, eg
— severe and persistent headache
— two distinct episodes of vomiting
5. a history of coagulopathy (eg warfarin use) and loss of consciousness, amnesia or any neurological feature.
CT scanning should be performed within eight hours in an adult patient who is otherwise well but has any of the following features:
1. age>65 (with loss of consciousness or amnesia)
2. clinical evidence of a skull fracture (eg boggy scalp haematoma) but no clinical features indicative of an immediate CT scan
3. any seizure activity
4. significant retrograde amnesia (>30 minutes)
5. dangerous mechanism of injury (pedestrian struck by motor vehicle, occupant ejected from motor vehicle, significant fall from height) or significant assault (eg blunt trauma with a weapon).
In adult patients who are GCS<15 with indications for a CT head scan, scanning should include the cervical spine.
Indications for admission to hospital An adult patient should be admitted/observed to hospital if:
1. the level of consciousness is impaired (GCS<15/15)
2. the patient is fully conscious (GCS 15/15) but has any indication for a CT scan (if the scan is normal and there are no other reasons for admission, then the patient may be considered for discharge)
3. the patient has significant medical problems, eg anticoagulant use
4. the patient has social problems or cannot be supervised by a responsible adult.
Referral to neurosurgical unit A patient with a head injury should be discussed with a neurosurgeon:
1. when a CT scan in a general hospital shows a recent intracranial lesion
when a patient fulfills the criteria for CT scanning but facilities are unavailable
2. when the patient has clinical features that suggest that specialist neuroscience assessment, monitoring, or management are appropriate, irrespective of the result of any CT scan.
3. All salvageable patients with severe head injury (GCS score 8/15 or less) should be
4. transferred to, and treated in, a setting with 24-hour neurological ICU facility.
Children Initial assessment
Great care should be taken when interpreting the Glasgow Coma Scale in the
under fives and this should be done by those with experience in the management of the young child. Pediatric Glasgow Coma Scale and Scoring (for use in patients under five years of age)
Pediatric Glasgow Coma Scale
Indications for referral to hospital In addition to the indications for referral of adults to hospital, children who have sustained a head injury should be referred to hospital if any of the following risk factors apply:
1. clinical suspicion of non-accidental injury
2. significant medical co-morbidity (eg learning difficulties, autism, metabolic disorders)
3. difficulty making a full assessment
4. not accompanied by a responsible adult
5. social circumstances considered unsuitable.
Indications for head CT scan Immediate CT scanning should be done in a child (<16 years) who has any of the following features:
1. GCS≤13 on assessment in emergency department
2. witnessed loss of consciousness >5 minutes
3. suspicion of open or depressed skull injury or tense fontanel
4. focal neurological deficit
5. any sign of basal skull fracture.
CT scanning should be considered within eight hours if any of the following features are present (excluding indications for an immediate scan):
1. presence of any bruise/swelling/laceration >5 cm on the head
2. post-traumatic seizure, but no history of epilepsy nor history suggestive –of reflex anoxic seizure
–amnesia (anterograde or retrograde) lasting >5 minutes
–clinical suspicion of non-accidental head injury
–a significant fall
–age under one year: GCS<15 in emergency department assessed by
–personnel experienced in paediatric GCS monitoring
–three or more discrete episodes of vomiting
–abnormal drowsiness (slowness to respond).
If a child meets head injury criteria for admission and was involved in a high speed road traffic accident, scanning should be done immediately
Indications for admission to hospital Children who have sustained a head injury should be admitted to hospital if any of the following risk factors apply:
1. any indication for a CT scan
2. suspicion of non-accidental injury
3. significant medical co-morbidity
4. difficulty making a full assessment
5. child not accompanied by a responsible adult
6. social circumstances considered unsuitable.
Referral to neurosurgical unit A patient with a head injury should be discussed with a neurosurgeon:
1. when a CT scan in a general hospital shows a recent intracranial lesion
2. when a patient fulfills the criteria for CT scanning but facilities are
unavailable
3. when the patient has clinical features that suggest that specialist
neuroscience assessment, monitoring, or management are appropriate,
irrespective of the result of any CT scan.
4. All salvageable patients with severe head injury (GCS score 8/15 or less) should be transferred to, and treated in, a setting with 24-hour neurological ICU facility.
In hospital care All medical and nursing staff involved in the care of patients with a head injury should be trained and competent in the use and recording of the Glasgow Coma Scale. The GCS should not be used in isolation and other parameters should be considered along with it, such as:
–pupil size and reactivity
–limb movements
–respiratory rate and oxygen saturation
–heart rate
–blood pressure
–temperature
–unusual behavior or temperament or speech impairment.
Family members and friends should be used as a source of information.
Observations should be recorded on a chart
Children <3 years old who have sustained a head injury are particularly difficult to evaluate and clinicians should have a low threshold of suspicion for early consultation with a specialist pediatric unit.
Children who are admitted should be under the care of a multidisciplinary team that includes a pediatric trained doctor experienced in the care of children with a head injury.
Children should be observed on a children’s ward.
The risk of rapid deterioration is greatest in the first six hours after injury and then decreases. If the patient is admitted on the first day of the injury then repeat evaluation every few hours is indicated if high risk factors such as high energy injury, Glasgow coma scale < 15, or focal neurological deficit is present.
Medical staff should assess the patient on admission to the ward and should re-assess the patient at least once within the next 24 hours. Assessment should include: examination for the GCS, neck movement, limb power, pupil reactions, all cranial nerves and signs of basal skull fracture.
Any of the following examples of neurological deterioration should prompt urgent re-appraisal by a doctor:
–the development of agitation or abnormal behavior
–a sustained decrease in conscious level of at least one point in the motor or verbal response or two points in the eye opening response of the GCS score
–the development of severe or increasing headache or persisting vomiting
new or evolving neurological symptoms or signs, such as pupil inequality or
asymmetry of limb or facial movement.
If re-assessment confirms a neurological deterioration, many factors need to be evaluated but the first step is to ensure the airway is clear, and that oxygenation and circulation are adequate.
Clinical signs of shock in a patient with a head injury should be assumed, until proven otherwise, to be due to hypovolemia caused by associated injuries.
Whilst an intoxicating agent may confuse the clinical picture, the assumption that deterioration or failure to improve is due to drugs or alcohol must be resisted.
If systemic causes of deterioration such as hypoxia, fluid and electrolyte imbalance, or hypoglycemia can be excluded, then resuscitation should continue according to accepted trauma protocols.
After traumatic brain injury, agitation may be a sign of neurological deterioration, hypoxia, electrolyte disturbance, drug/alcohol withdrawal, or seizures. Medical evaluation should be done in conjunction with pharmacological therapy for behavior.
Therapeutic Goals and Interventions
Systolic BP < 90 mm Hg and O2 Saturation < 90% should be avoided.
Mannitol
Mannitol in doses of 0.25gram/kg to 1.0gram/kg may reduce ICP. Our usual regimen is to give an initial dose of 1.0 gram/kg and the start 0.25mg/kg every 8 hours. The dose can be increased up to 1.0 gram/kg and frequency up to every 6 hours as needed. It is most useful as a temporizing measure such as to treat a patient suspected of having a mass lesion which may be surgical while preparing that patient for surgery. It is most effective in bolus doses rather constant infusion which may be repeated every 6 hours. Most of the world wide experience deals with controlling intracranial pressure which is being monitored. It should not be a part of routine head injury management. Side effects of hypotension, increases in size of intraparenchymal brain hemorrhage, and kidney dysfunction may occur.
The use of mannitol for head injury treatment in developing countries without ICP monitoring has not been well studied.
Indications:
1. Salvageable Head Injury with GCS 8 or less.
2. Deterioration from GCS > 8 to less for three days as above
3. Pre-operative .25gram/kg to 1.0gram/kg dose for suspected or known mass lesion. May be repeated intra-operatively.
4. Post-operative management of cerebral edema
Enteral feeding should be begun by 72 hours after injury. Hyperglycemia should be avoided as increased intracellular lactic acidosis can worsen brain injury.
Seizures and Seizure Prophylaxis
Prophylactic anticonvulsants does not reduce late seizure development or improve outcomes. However we face an unusual situation in Ethiopia where there are no intravenous anticonvulsants. We have had experiences of a few patients in the past few years whose developed early onset post traumatic seizures which where difficult to control while we were waiting for oral phenytoin to be absorbed which typically takes about 24 hours. Therefore we are changing our previous recommendation to start phenytoin or carbamezipine in any patient with an abnormal brain finding on CT Scan of the brain and continue for 7 days.
Anticonvulsant treatment indications:
Phenytoin use according to body mass and age for a seizure in the first few days and continued for one week.
Craniotomy for intraparenchymal lesion (evacuation of hemorrhagic contusion or lobectomy) or if a dural tear is discovered such as for depressed fracture
Infection Prophylaxis
Routine single dose of Ceftriaxzone 1 gm IV on call for adults and 50mg/Kg in children for closed head injuries requiring surgery.
Single dose of periprocedural antibiotics for intubation only unless the patient has signs of aspiration pneumonia already present.
DVT Prophylaxis
Low molecular weight heparin is contraindicated in the presence of acute head injury. If there is no large hematoma (intraparenchymal) then generally should wait at least five days before beginning low dose heparin 5,000 units BID or low molecular weight heparin Graduated stockings or pneumatic compression stockings if available are appropriate.
Hyperventilation
Profound hypercarbia may increase ICP and profound hypocarbia may decrease cerebral perfusion. Hyperventilation is to be avoided in the first 24 hours after injury. Temporary mild hyperventilation pre-operatively or intra-operatively may be used.
Steroids
There is no sound scientific evidence supporting the use of steroids for head injury.
Barbiturates
Under special circumstances such as post-operative swelling or diffuse cerebral swelling in a viable patients in consultation with neurosurgical staff pentobarbital at 3mg/kg/ hour may be given for up to three days to attempt to control brain swelling. Patients who have bilateral dilated pupils and decreased brain stem function are not candidates for this treatment modality.
Post-Traumatic Meningitis
Most of the studies suggest post-traumatic meningitis can be treated similar to community acquired bacterial meningitis with Ceftriaxzone 1 gm Q12h in adults. If no response is seen consideration can be given to adding Vancomycin and Meripenum for resistant organism. In our experience most patients respond to a 10 day course of Ceftriaxzone. Consideration can be given to performing a lumbar puncture for culture and sensitivity if CT Scan shows no mass effect. If staph aureus is identified then treatment should be extended for 21 days duration.
Surgical Management Guidelines
Note: The clinical progression of the patient must always be considered strongly in decision to do surgery or treat conservatively. Lesions affecting the temporal lobe area are at high risk of rapid deterioration especially within the first three days after injury.
Epidural hematoma
–An epidural hematoma greater than 30 cm squared should be evacuated regardless of GCS score
–An epidural hematoma less than 30 cm squared, midline shift less than 5mm, and thickness less than 15 mm in a patient without neurological deficit can usually be considered for nonsurgical treatment if clearly clinically stable
–Acute epidural hematoma is best treated by craniotomy rather then burr holes. Tacking up of the dura to prevent rebleeding should be done.
Acute Subdural Hematoma
–An acute subdural hematoma with a thickness greater than 10 mm or midline shift greater than 5 mm should be evacuated regardless of GCS score
–Patients who have a large parenchymal contusion and acute subdural less than 10mm with an admission GCS< 9 and then subsequent deterioration may be a candidate for surgery.
–In severe cases of brain swelling. Bone flap removal and duraplasty may be necessary.
Surgery for Traumatic Intraparenchymal Lesions
–Surgery for resection of intraparenchymal lesions is not within the normal procedure guidelines for general surgery.
–Patients with focal intraparenchymal lesions who present with a GCS of 8 will be initially placed on medical management protocols.
–Patients with a GCS of 8 who deteriorate despite medical management will be discussed with the neurosurgical staff as regards to management
Chronic Subdural Hematoma
–A totally asymptomatic patient with evidence of a chronic subdural hematoma may be conservatively followed
–A symptomatic patient with chronic subdural hematoma should undergo timely operation
–The best outcome in chronic subdural hematoma was found in a prospective study utilizing the two burr hole technique with subdural drain placement. At Ayder an initial burr hole will placed frontally or parietally depending upon where the greatest thickness of the hematoma is found. If after irrigation of the subdural space the brain does not expand to the dura then a second burr hole will be placed. If the clot is gelatinous then the burr holes will be converted to a craniotomy. A pediatric feeding tube will always be place in the subdural space at least one centimeter beyond the proximal last side hole and exited through a separate stab wound.
–The subdural drain may be removed when the old blood drainage converts to CSF. The drain should be removed by the morning of the third day after surgery.
–After surgery while the subdural drain is in place the patient’s head should be kept flat to maximize brain re-expansion which will push out the remaining subdural hematoma
–If patient deteriorates following surgery after initial improvement or fails to improve then consideration for a repeat CT scan should be done.
Closed Depressed Skull Fracture
–Patients with a closed depressed fracture with a depression less than 1 cm and no neurological findings or associated hematoma requiring surgery are potential candidates for conservative treatment
–A closed depressed fracture with a depression 1 cm or greater (which is deeper then the inner table) and/or neurological deficit should under go timely surgical intervention.
–Patients with simple depressed fractures without dural tear or cerebral contusion require only routine pre-operative antibiotic prophylaxis and no anticonvulsant prophylaxis.
Open Depressed Skull Fracture
–Patients with an open depressed fracture greater than the depth of the calvarium should undergo surgery.
–Operation should be done within the first 48 hours after injury to reduce the risk of infection.
–The bone flap or fragments should be cleaned with betadiene and saline thoroughly before replacement
–A water tight closure of the dura should be attempted..
–Debridement of nonviable and contaminated brain should be done.
–A 24 hour course of intravenous Ceftriaxzone and Metronidazole should be given for cases where there is only minimal contamination and the dura is intact. Patients will then receive a 7 day oral course of Amoxicillin and Clavulanate (Augmentin) 500 mg every 8 hours for adults.
–An 7 day course of intravenous Ceftriaxzone and Metronidazole should be given for cases where there is extradual purulence, gross contamination or penetration of the brain especially if surgery was delayed more than 48 hours after injury.followed by a one week course of Augmentin orally.
–Post traumatic cerebritis or abscess requires 6 week course of intravenous antibiotics.
–Anticonvulsant prophlaxis should be given to all patients with dural laceration and open brain injury.