The following statement and plea is from the medical staff and other health care professionals from Mekelle University Ayder Comprehensive Specialized Hospital in Tigray. Normally this is a tertiary hospital serving over 10 million population of Tigray, Afar, northern Amhara, and refugees from Eritrea. The complete blockade of supplies, power, internet, telephone, and travel has rendered the hospital essentially inoperative.
Hoping Against Hope!
Jan. 4/ 2022: Position Statement of Doctors and other health professionals of Ayder Comprehensive Specialized Hospital – College of Health Sciences, Mekelle University
We, the Doctors and other health professionals of Ayder Comprehensive Specialized Hospital – College of Health Sciences, at Mekelle University, hear and experience firsthand the daily suffering our patients are enduring. As we had solemnly sworn an oath to protect and save our patients from suffering, the least we could do on difficult days like these ones is to become their voice and ventilate their sufferings for the world to hear.
The statement below, therefore, is the collective voice of all of us working in the hospital and the college to echoing our patients’ plea that we hear every day for the last six months.
We have no doubt that anyone listening or reading this position statement will be cognizant of the fact that meeting the health needs of a community in low-resource settings such as ours is a very daunting endeavor, even in times of peace and stability.
To substantiate this, we wish to put some historical milestones of our college into perspective:
• We, the Doctors and other Health Professionals of Ayder Comprehensive Specialized Hospital – College of Health Sciences, remember our humble beginnings 14 years ago. We remember that, back then, our 500 – bed hospital had stood empty and idle for nearly a decade because of the severe shortage of health professionals, medical instruments, and financial resources.
• We also remember how this once empty hospital had grown fast through the hard work and perseverance of all of us, the unwavering support of our university, national and international partners.
A hospital that was barely better than a countryside health post in the early days of its establishment, grew to be a specialized referral center a decade later serving a catchment area of 9 million people from Tigray, neighboring districts of the Afar and Amhara regions.
It won’t be forgotten that our hospital had been also serving Eritrean refugees staying in the camps in Northern Ethiopia for quite a while. It is also to be well remembered that patients from Eritrea were well taken care of in our hospital during the brief period of border normalization between our two countries in 2018.
Our hospital’s annual patient visit had risen to nearly 300,000 and thousands of major surgeries, deliveries, and a wide variety of interventions and treatments used to be given.
We all took those positive developments for granted and it was customary for us to focus on future progress rather than dwell on past achievements.
However, while mentally unprepared, we have found ourselves, in such a short period of time, in a situation that we would never ever have considered possible in our wildest imaginations. How could we ever have expected to cancel surgeries for lack of intravenous fluids, anesthesia drugs, or tell patients or their relatives to find intravenous fluids somewhere in the city while the patient needed quick support?
But, we have been forced to work in a hospital without intravenous fluids, gloves, even the most commonly used antibiotics, anti-pain medications, drugs vital for women undergoing labor and delivery, drugs for various kinds of mental illnesses, basic laboratory tests, and a lot more other essential drugs.
• The availability of essential drugs, which was 79.3% a couple of years ago and 82% a year ago has now gone down to 17.5%.
• The availability of laboratory tests which was 93.7%, a couple of years ago and 84.2% a year ago, has now gone down to 42.1%.
The numbers are going down rapidly every week. The oxygen supply to our hospital has become very unreliable and resulted in the death of patients because of the frequent breaking down of the machines that could have been easily repaired if we got spare parts from the manufacturer through Addis Ababa to Mekelle which is now completely impossible.
To make matters worse, electricity blackouts have become more common and prolonged for days at times. There is no means of communication within the hospital and beyond. Thus, we have to walk and find the person we need, even to do something trivial.
We, the staff of the hospital and the college haven’t lost hope despite the huge psychological burden that we have to deal with as a result of witnessing what is happening to our patients on a daily basis.
As you might all be aware of:
• We haven’t been paid our well-deserved salaries for the last seven months, our extra–time payments for nearly 13 months,
• We are unable to withdraw whatever amount of money we have had in governmental and private banks because of the complete shutdown of banking service
• We have nothing to feed our families and ourselves
Against all odds, however, we have continued to serve our patients with whatever supplies are at our disposal!
We have:
• tried to produce fluids locally to clean infected wounds,
• beg business people or residents in the city to give us detergents, soap, bed sheets, and other linen for free or on credit to be able to keep the hospital running.
We have used and are still using expired drugs when that is the only option left. We have tried to give care to those in the most urgent need and ask others to wait to know that those who are waiting are also getting closer to hapless conditions.
Our neurosurgery team has decided to operate on patients with problems in the brain just based on clinical examinations, without having the support of CT scan and/or MRI images which have both been not functional for many months because spare parts could not reach our city due to the complete blockage.
Supplies that we used to get for free from donors and partners, as well as business counterparts, have not reached our hospital for the last six months.
As a result, children who needed shunt surgeries are left to die, those with treatable cancers are denied their rights and those with fractures are forced to wait while being immobilized.
Those who could easily have been saved with hemodialysis are dying. Patients who have had dialysis for years at our hospital are forced to die just because the supplies that could have been brought are not allowed to reach us.
The world is tested with COVID19. Add a large-scale, full-fledged War on it. Then add a siege on it. Imagine this three combined in a poor region that struggles for survival even in times of peace and stability.
We earnestly believe that there are very good people out there in Ethiopia, the horn of Arica, Africa, and the rest of the world who could be the advocates of our patients, our health professionals, and our people. We wonder how the world lets this man-made crisis continue unabated while it has all the capacity and the means it needs to stop it.
We, therefore, humbly and respectfully request all health professionals in Ethiopia, Africa, and the world to be the voice of our patients and stand with us in our effort to end the crisis. We also request the Ministry of Health of Ethiopia, different UN and other international organizations, all the other local partners, NGOs as well as international partners to intervene and bring the misery of several months to an end.
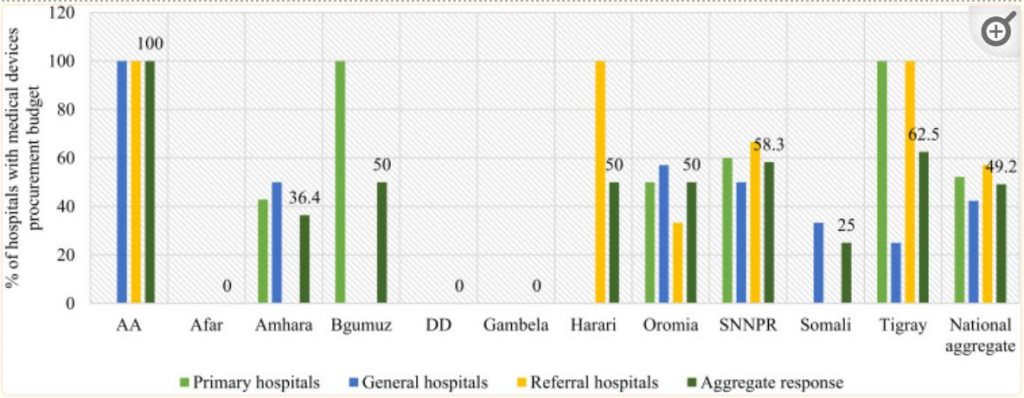
Whatever the cause of the war is, it cannot be right or ethical to deny patients lifesaving health care. Neither can it be justified to completely withhold a hospital budget for several months as if it is never the responsibility of the government of Ethiopia to let a hospital carry on its activities and deliver health to innocent civilians in urgent need of care.
We, people in the world, live on a tiny planet and our destinies are intertwined. It would be very heartbreaking to see those with the power and capacity do nothing except viciously say that they are “concerned”, “very concerned”, and “gravely concerned.”
It is already very late but those national, continental, and global authorities in health, as well as governments and organizations responsible for solving such problems, can still avert a catastrophe.
We have seen the world do that before and we, your fellow brothers and sisters, believe and hope against hope that you will do the same this time around as well.
Doctors and other Health Professionals of Ayder Comprehensive Specialized Hospital – College of Health Sciences, at Mekelle University