
The Mekelle University Multidisciplinary Research Group for Neural Tube Defects has just published its first research paper in Brain & Development Journal July 2018, “Maternal Risk Factors Associated with Neural Tube Defects in the Tigray Region of Ethiopia”. This being the first major prospective study done on neural tube defects in Ethiopia confirmed our worst fears of a very high incidence, significantly higher than the 75 per 10,000 births seen in most of Sub-Saharan Africa. There a many challenges in how this problem can be addressed involving cultural beliefs and practices, poverty, diet diversity, supplementation, and fortification. Unfortunately, applying a Western style solution for Ethiopia will not be so easy or likely to succeed as well.
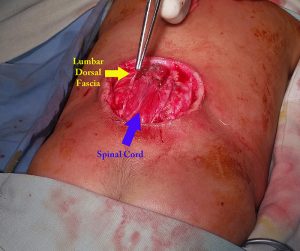
For the past decade the development of neurosurgery in Ethiopia has witnessed the high incidence of neural tube defects including myelomeningocoel and anencephaly coming to their clinics first in Addis Ababa but now also in Mekelle, Gondar, Bahir Dar, and Oromia. Previous published reports noted incidences first of greater than 160 per 10,000 births in Addis with a more recent report of 191 per 10,000 births in Addis Ababa. The reports of up 300 per 10,000 in some areas of Tigray are higher than those reported in any other developing countries.
Research replicated in nine countries in the 1960s and 1970s showed that neural tube defects were somewhat but no totally related to lack of folic acid in the diet and that adding folic acid would significantly reduce the incidence of neural tube defects. At first attempts were made with prescribing supplementation for women of childbearing age but this did not have the desired result. The incidence really came down in Europe and the United States when the government mandated the fortification of folic acid in food staples like bread and cereals
One of the factors we identified was that a lack of diet diversity increased the risk for NTDS while increased diversity reduced it. About 65% of the diet of most Ethiopians is enjera bread made at home from teff and boiled chick peas called shiro. Although a serving of raw chick peas has about 1000 micrograms of folic acid its likely that boiling them reduces the folic acid to basically nothing. A similar situation exists for spinach which is often boiled and eaten during the rainy season.
Traditionally, Ethiopians avoid eating fresh vegetables and fruits as documented in our study and many previous others. In fact a study of the one hundred most elite Ethiopian runners showed that 20% had a significant folic acid deficiency which correlated with lack of dietary diversity (avoiding greens and fruit). In the countryside where the women may spend many hours a day just to get 5 gallons of water, there is not much water to spare for cleaning produce. The population fears getting diarrheal illness from such produce.
Our study showed that of more than 13,000 women interviewed who were pregnant essentially none of them had any knowledge of preconceptional nutritional needs or about neural tube defects.
Convincing Ethiopians to take medication for invisible illness such as hypertension has proved difficult. Research in many parts of Ethiopia has shown for example that as few as 50% of those prescribed medication for hypertension actually take it. There exists underlying fears of addiction to “un-natural” substances. Will Ethiopian women be convinced to take supplementation?
Ethiopians especially the 88% who live in country side rarely buy food staples like bread but instead make their own enjera from stored teff. Currently there is only one factory in the country capable of making fortified bread but it is not functioning.
The cost of a months supply of folic acid 4 milligrams per day is about 80 birr or about $2.40 US for a single woman. Given the fact that the average family makes about 250 birr per month to support a family of six, there is little room to allow payment of this expense. There are no current domestic producers of folic acid so considerable hard foreign currency would need to be mobilized to import stock. For the government to provide this for every women of child bearing age would cost tens of millions of dollars to be added to the budget of a country which currently spends the equivalent of about $13 per capita for the 100 million population.
Ultimately addressing the issue of the high incidence of neural tube defects in Ethiopia will be requiring taking into account cultural norms and practices in such a way that changes are seen as consistent with Ethiopian culture. Widespread public education and a major investment in folic acid purchases by the government will be necessary. This begins with the clear realization that there is a problem.